Detail your services
Display real testimonials
Display real testimonials
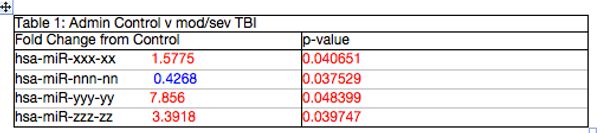
Four miRNAs are altered in moderate to severe TBI. Ten moderate to severe TBI subjects with a GCS<12 had blood drawn upon entry to the emergency department. The results of their initial draw are shown in table 1. Clearly, there are significant differences in miRNA present in the moderate to severe TBI group. Of interest, these are the same miRNA that were altered in a subset of the mild TBI football and soccer players presented in figure below.
Display real testimonials
Display real testimonials
Display real testimonials
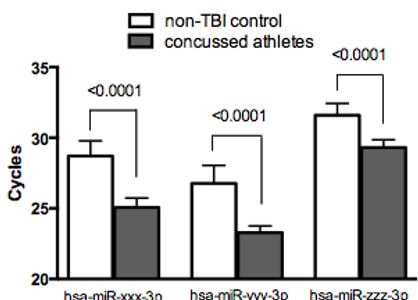
Three miRNAs shown are significantly altered following repeated mild TBI in male football and female soccer players. Seventy-seven athletes had blood drawn prior to the beginning of their respective seasons. Of this group, 17 individuals self-reported having persistent symptoms following a concussion (headaches, difficulty concentrating, and insomnia). However, none of the 17 athletes had suffered a concussion in the 6 months prior to testing. At the time of the blood draw none of the athletes had any TBI associated symptoms present. Results from our analysis clearly show these 17 athletes were significantly different from other athletes or non-TBI controls. These results suggest a sub-population of athletes (22%) may be vulnerable to mTBI and may experience long-term effects that occur at a molecular level. Athletes (13 males and 4 females) mean athlete age=22 years. Non-TBI controls (6 males, 9 females) mean age of 31. Two-tailed T-test was used for each comparison.
Four miRNAs are altered in moderate to severe TBI. Ten moderate to severe TBI subjects with a GCS<12 had blood drawn upon entry to the emergency department. The results of their initial draw are shown in table 1. Clearly, there are significant differences in miRNA present in the moderate to severe TBI group. Of interest, these are the same miRNA that were altered in a subset of the mild TBI football and soccer players presented in figure below.

Three miRNAs shown are significantly altered following repeated mild TBI in male football and female soccer players. Seventy-seven athletes had blood drawn prior to the beginning of their respective seasons. Of this group, 17 individuals self-reported having persistent symptoms following a concussion (headaches, difficulty concentrating, and insomnia). However, none of the 17 athletes had suffered a concussion in the 6 months prior to testing. At the time of the blood draw none of the athletes had any TBI associated symptoms present. Results from our analysis clearly show these 17 athletes were significantly different from other athletes or non-TBI controls. These results suggest a sub-population of athletes (22%) may be vulnerable to mTBI and may experience long-term effects that occur at a molecular level. Athletes (13 males and 4 females) mean athlete age=22 years. Non-TBI controls (6 males, 9 females) mean age of 31. Two-tailed T-test was used for each comparison.
Our published studies till now;
1. Mitra B, et al. Plasma micro-RNA biomarkers for diagnosis and prognosis after traumatic brain injury: A pilot study. J Clin Neurosci (2017), http://dx.doi.org/10.1016/j.jocn.2016.12.009
2. Diane M, et al. Multiple mild traumatic brain injury in the rat produces persistent pathological alterations in the brain Exp. Neu (2017), http://dx.doi.org/10.1016/j.expneurol.2017.07.015
3. Rau T, et al. Efficacy of a repeat testing protocol for cognitive fatigue assessment: a preliminary study in postconcussive syndrome participants. Concussion (2017) https://www.futuremedicine.com/doi/suppl/10.2217/cnc-2017-0002
4. Mitra B, et al. Micro-RNA levels and symptom profile after mild traumatic brain injury: A longitudinal cohort study. J Clin Neuroscience (2021), https://doi.org/10.1016/j.jocn.2021.11.021
5. Mitra B, et al. MicroRNA biomarkers for diagnosis of mild traumatic brain injury and prediction of persistent symptoms: A prospective cohort study. J Clin Neuroscience (2023), https://doi.org/10.1016/j.jocn.2023.07.011